Diagnosis of Acute ACL injuries
Natural history of the ACL deficient knee
What does it take to replace the human ACL?
- Biomechanical considerations
- Graft selection factors
- Biology of graft healing
- Graft placement
- Graft tension
- Graft fixation
Surgical Technique
Diagnosis
The history of a patient who has sustained an acute injury to the ACL is fairly typical. Most “isolated” ACL injuries occur as a result of a non contact, deceleration, twisting, or pivoting type mechanisms. Many patients will describe a feeling of the joint “going out of place”, and approximately 40% 60% will feel or hear a “pop” at the time of the injury. The injury is followed by an inability to continue playing, and joint swelling within 24 hours. Any patient who gives a history similar to the above should be suspected of having a ACL injury until proven otherwise.
After obtaining a thorough history, physical examination of the knee is performed. The ease of examination often depends on the timing of the examination. If the patient is examined soon after the injury and before a large joint effusion and muscle spasm have occurred, it is relatively easy to perform an adequate ligament examination. On the other hand if the examination is performed days after the initial injury, when the knee is swollen and painful, and the muscles are in spasm, ligament examination can be very difficult.
Although it is important to perform a complete examination of the knee, the hallmark of a ligament injury is the presence of pathological knee motion. Numerous biomechanical studies have shown that the ACL is the primary restraint to anterior tibial translation, providing approximately 85% of the resistance to anterior tibial translation. Transection of the ACL leads to an increase in anterior tibial translation. Clinical and biomechanical studies have confirmed that the amount of anterior tibial translation is greater at 20° 30° than at 90° because of the stabilizing effect of the secondary restraints at 90° (principally the posterior horn of the menisci). Therefore the Lachman test, is a much more sensitive test than the anterior drawer test to diagnose an ACL tear. Studies by Dale Daniel have also shown that further sensitivity can be obtained by also noting the quality of the endpoint. A intact ACL is confirmed by the presence of a hard, or firm endpoint, while the torn ACL is characterized by a soft, or indistinct endpoint. Clinical studies have shown that using these criteria, an experienced clinician can achieve approximately a 90% accuracy rate in diagnosing an ACL tear.
The collateral ligaments are assessed by performing valgus, and varus rotations with the knee hyperextended, at 0°, and between 20° 30°. The posterolateral structures are tested by assessing external tibial rotation at 0°, 30°, and 90°. Biomechanical studies indicate that the PCL is best tested with the knee flexed to between 70° 90°, but this is often difficult to do in the acute knee because of pain.
Rotational tests such as the pivot shift test (click on video), and the reverse pivot shift test are an important part of the examination in the chronic knee, but because they produce pain in the acute knee they can be difficult to perform. The flexion rotation drawer test (FRD) as described by Noyes, provides similar information as the pivot shift test, and can often be performed in the acute knee.
Following clinical examination of the knee, appropriate laboratory studies are performed. All patients with acute knee injuries should have as a minimum, routine AP, Lateral, and Skyline radiographs of the injured knee. The role of MRI in the management of acute knee injuries is controversial. MRI studies can provide highly accurate information on the status of the cruciate ligaments, the collateral ligaments, the menisci, the subchondral bone, and the articular cartilage. The disadvantage of MRI is the high cost. As mentioned earlier, the diagnosis of an ACL tear should be able to be made on the basis of the history, and clinical examination of the knee, so in most cases MRI is not needed to tell the surgeon that the ACL is torn. Where MRI is clearly superior, and has a role to play is in the diagnosis and management of meniscal injuries.
Most clinical studies have documented a high rate of associated meniscal injuries with an acute tear of the ACL. Approximately 40 % 60 % of patients presenting with a acute ACL’ tear will have an associated meniscal injury. In many cases the management of the meniscal tear will determine the need for ACL surgery. For instance, it has clearly been documented that the healing rate for repairable menisci is improved with concomitant ACL reconstruction, so most surgeons now advise that if meniscal repair is going to be considered that ACL reconstruction be performed as well. By detecting meniscal injuries, MRI can provide valuable information for both the patient and the surgeon.
Natural History of the ACL Deficient Knee
So far, there has yet to be a true natural history study of the untreated ACL injury. Limitations of present studies include the following: (1) most are retrospective studies (2) most contain different injury patterns not just “isolated” ACL injuries (3) different patient populations (4) lack of a uniform grading scale to document what is a successful result. Although most of the recent studies are not true “natural history” studies, many of them have shed some light of some of the problems that can occur following a ACL tear. Injury to the ACL causes a functional disability which is variable in nature. In its most severe expression, loss of the ACL causes repeated giving way episodes, which leads to meniscal tears, chondrosis, and ultimately degenerative arthritis, the so called “ACL syndrome”. This functional instability is most likely to occur in patients who participate in athletic activities involving cutting, pivoting, jumping, acceleration, and deceleration.
The outcome following a tear of the ACL is also amplified by various risks factors listed below. Analysis of the patients risk factors will help the clinician decide which patients are most at risk for developing functional instability, and help guide management.
ACL Risk Factors for Acute Patients
- Young athletic patients wishing to return to pivoting, jumping, cutting sports (basketball, volleyball, soccer, gymnastics)
- Knee type:
ACL dominant knee
Thin, weak secondary restraints Hyperextension (loose jointed)
The ACL is the predominant anterior translational restraint with little contribution from the secondary restraints.
Quadriceps dominant kne
Sports like basketball, volleyball, soccer, gymnastics. Because of the large quadriceps forces the secondary restraints quickly stretch out. - Grade III (10 15 mm) or IV (> 15 mm) anterior tibial subluxation.
- Meniscal injury
- Chondral injury
- Varus alignment, varus laxity, varus recurvatum (Varus, double varus, triple varus knee)
Risk Factors for Chronic Patient
- Recurrent giving way episodes
- Failure to modify activities
- Grade IV laxity pattern
- Meniscal damage
- Tibiofemoral crepitus
- Patellofemoral changes
- Chondral fracture
- Varus knee
- Generalized ligamentous laxity
Who should have an ACL Reconstruction
Acute Cases
- Active patient who wishes to continue to participate in sports which involve jumping, landing, pivoting and twisting.
- ACL + Grade III collateral ligament injury.
- ACL + meniscus tear
- ACL + osteochondral or chondral damage.
- MIRF (Meniscus injury risk factor) > 3.
Chronic Cases
- Patients with functionally disabling giving way episodes who are unwilling to modify their lifestyle.
- 2. Giving way with ADL.
- 3. ACL + repairable menisci.
What does it take to replace the human ACL?
Biomechanical Factors for the Human Anterior Cruciate Ligament:
Strength: 1725 ± 269 Newtons (Noyes data) . Data from Woo et al.” indicate a higher value of 2160 ± 157 Newtons. Length: 26.9 ± 1.1 mm Area: 44.4 ± 4.0 mm Stiffness: 175 N/mm (Noyes data ). 242 ± 26 N/mm (Woo data) Elongation at failure: 15%
Estimated Loads Experienced by the ACL During ADL
- Activity Maximum Force (N)
- Level Walking 210
- Ascending Stairs 67
- Descending Stairs 133
- Sitting and Rising 173
- Ascending Ramp 107
- Descending Ramp 485
- Jogging 630
- Jolting 700
Cycles per year: Approximately 4 million
Biomechanics of ACL Reconstruction
Mechanical Properties of ACL Graft substitutes
Noyes, Butler, Grood: Biomechanical Analysis of Human Ligament Grafts Used in Knee Ligament Repairs and Reconstructions. Journal of Bone and Joint Surgery. 1984.
Autograft
TISSUE STRENGTH (N) % OF ACL STRENGTH WIDTH (mm)
ACL 1725 ± 269 100%
Bone Patellar
Tendon Bone
Central 1/3 2900 ± 260 168% 13.8 ±1.4
Medial 1/3 2734 ± 298 158% 14.9 ±1.1
Semitendinous 1216 ± 50 70%
Fascia Lata 628 ± 35 36% 15.6 ±0.8
(15 mm)
Fascia Lata 1800 104% 45
(45 mm)
Gracilis 838 ± 30 49%
TISSUE STRENGTH (N) % OF ACL STRENGTH WIDTH (mm)
Central 1/3
Patellar Tendon 2977 ± 516 173% (Noyes data) 10 mm
138% (Woo data)
2238 ± 316 130% (Noyes data) 7 mm
104% (Woo data)
Quads Tendon Similar to Patellar Tendon
4x Hamstring graft 4158 + 221 242% 8-9 mm
Rotation of the graft by 90° increased the ultimate failure load of
all grafts by approximately 30%. This study suggests that smaller
width (9 10 mm) patellar tendon grafts can be used for ACL
reconstructions. In BTB Reconstruction a size of 9-10 mm is usually used. The graft strength of a patellar tendon graft is about 30% less compared to a quadruple hamstring graft. Quads Tendon strength is similar to Patella Tendon.
ACL Graft Selection
- Autografts
- Patellar tendon
- Hamstring tendons
- Quadriceps tendon
- Allografts
- Achilles tendon
- Patellar tendon
Prosthetic(LARS)
Although the initial biomechanical properties of ACL grafts play a major role in the success of ACL reconstruction, the knee surgeon must also consider the surgical morbidity of harvesting the graft tissue, morbidity resulting from the loss of the graft tissue, the initial fixation strength, and the healing potential of a particular graft.
Patellar Tendon
1.Most commonly used in the past. Was Considered by some surgeons to be “the gold standard” for autografts.
Advantages
- High initial tensile strength
- Bone to bone fixation provides excellent initial fixation strength and stiffness
- Bone to bone healing
Because of the above properties patellar tendon grafts require less postoperative protection in the early postoperative period prior to biological incorporation of the graft fixation sites.
Disadvantages
- Increased incidence of donor site complications (donor site pain, patellar tendinitis, patellar tendon rupture, patellar fracture, quadriceps weakness, patellofemoral pain, inability to kneel)
- Much stiffer than the normal ACL
- Associated with a greater incidence of arthrofibrosis, patellar entrapment and loss of motion compared to hamstring tendon grafts, and allografts
- Higher risk of Patello femoral Osteoartritis
Hamstring Tendons (Semitendinous and Gracilis)
Can be used as single stranded or double stranded grafts.
The 4x Hamstring Tendon graft has around double the strength of a normal ACL.
Due to the high initial graft strength and the low morbidity, the quadruple hamstring graft has become my graft of choice.
Advantages
- Lower incidence of donor site complications and morbidity
- More closely matches the stiffness of the normal ACL.
- Associated with a lower incidence of arthrofibrosis, patellar entrapment and motion problems, as well as ability to kneel
- High initial graft strength (+ 4000 Newton !) and fixation strength (+ 1000 Newton!)
Disadvantages
- At the introduction of HS tendon graft for ACL reconstruction, some authors claimed the HST graft to be weaker compared to Patella tendon, however through biomechanical experiments it has been proven , that the graft strength is in actual fact 30 % higher compared to a Patellar tendon graft. Elasticity of the HST graft is more close to the normal ACL vs Patella tendon Graft, which is stiffer.
- Lower initial graft fixation strength was also quoted , however with current fixation options, Endobutton CL for femur and Intrafix for tibia, fixation strength of more than 1000 N can be achieved which is double the fixation strength of the Kurosaka IF screw with BTB graft.
- Soft tissue to bone healing vs bone to bone healing in Patella tendon Graft. Using an Interference screw, Weiler was able to show sharpeys fibres for hamstring fixation with direct tendon to bone healing (without fibrous interzone) as of 6 weeks. The healing time for hamstrings in the bone tunnel is usually 12 weeks compared to 6 weeks for BTB grafts.
Quadriceps Tendon Graft
Advantages
- High initial tensile strength (3100N Staeubli)
- Reduced Morbity compared to Patella Tendon
- Associated with low incidence of Arthofibrosis , Patella entrapment and motion problems , Ability to kneel
- Similar strength to Patella Tendon Graft
Disadvantages
- Scar on top of the knee not as nice
- Soft tissue to bone healing similar to Hamstring Tendon / using IF screw Fixation. Direct Tendon to Bone healing without fibrous interzone (Weiler 1999)
Allografts
Advantages
- No donor site morbidity.
- Unlimited size.
Disadvantages
- Disease transmission. AIDS estimate 1 in 1.5 million.
- Variability in “tissue bank” standards.
- Effects of secondary sterilization on the initial material properties
Irradiation
Disadvantages
- Radiation
> 2.5 Mrads decreases graft strength
Delamination of collagen
Ethylene Oxide
Induces adverse reactions “applesauce reaction”
Cystic changes around the bone tunnels - Bone bank standards very different
- Slower rate if biological incorporation compared to autografts
- Higher failure rate compared to autografts (click on J Buelow Poster )
Prosthetics (LARS)
Advantages
- No donor site morbidity.
- Availability.
- Rigid fixation possible.
- Rapid rehabilitation.
Disadvantages
- Cost.
- High long term failure rate.
- Higher infection rate.
- Abrasion and impingement can lead to “sterile” effusions.
- 30% poor results at 2 years (Australian Knee Society 2013)
- Lars ACL only for select cases and for clinical studies
- In many countries not permitted for intra-articular use because of high failure rate
As you can see each graft material has its advantages and disadvantages so one must decide on an individual basis which graft material is most appropriate for a given patient.
Graft Selection Factors
Prospective studies comparing the clinical outcomes of patients who underwent ACL reconstruction with patellar tendon autografts versus hamstring tendons, have shown there was no significant difference between the two grafts as far as knee stability is concerned. These studies suggest that both grafts sources can provide similar clinical outcomes. The challenge to the clinician is to try to determine situations that might favor one graft source over another in a particular patient. The Quadriceps Tendon Graft can provide similar outcomes compared to Hamstring and Patella Tendon Graft. Because of its advantages compared to the Patella Tendon, I favour the Quadriceps Tendon Graft over the Patella Tendon Graft.
In general, I see no indication for an artificial Graft. The risk of failure is, in my opinion, too high. In most European countries artificial ligaments like the Lars are not allowed to be used for ACL reconstruction.
In chronic patients with extreme degrees of laxity and stretching of the secondary restraints, a stiffer graft such as the Quadriceps or patellar tendon may provide an advantage compared to hamstring tendon grafts.
These advantages of the Quadriceps or Patella tendon graft must be balanced against the increased donor site morbidity which can be significant in some patients.
Hamstring tendon grafts would seem to be favored in acute patients where the secondary restraints are intact (or healing).
Hamstring tendon grafts are favored in patients who must kneel or crawl as part of their job requirement (eg. electricians, plumbers, carpenters), since an incision over the tibial tubercle and patella can be avoided reducing graft site pain. Hamstring tendon grafts are also favored in patients with patellofemoral pain or extensor malalignment problems, and patients who participate in quadriceps dominant sports such as basketball, track and field and volleyball. Most of those advantages do also apply for the Quadriceps tendon comparing it to the Patella Tendon Graft.
Allografts should be reserved for revision ACL reconstructions, multiple ligament cases reconstructions. Prosthetics have no indication, neither as Augmentation nor as ACL substitute. The Quadriceps tendon is a good alternative to the Patella Tendon with the advantage being that patients can kneel.
Hybrids (Combination of Lars Prosthetic with autologous hamstring tendon graft) are controversial. The hope and idea behind it is that there is potential longterm benefit from the hamstring tendon and a short term benefit (initial stiffness) from the Lars ligament. The problem is however that stress shielding of the hamstrings might weaken the hamstrings. The Lars component is likely to tear in the medium or longterm and this has potential risks including sterile effusions, Arthitis , increased risk for infection and more difficult revision surgery. The idea of an artificial Ligament is not new and in the literature, plenty of evidence suggests that a bad outcome can be expected, when an artificial Ligament is used for an ACL Reconstruction.
Biology of Graft Healing
The ultimate success of any biological intra articular reconstruction depends on the ability of the biological tissue to survive and maintain its initial biomechanical properties in the intra articular environment of the knee. Animal models have demonstrated that autografts are “free grafts” at the time of their implantation. The graft undergoes a complex biological process of necrosis, followed by revascularization, cellular repopulation, collagen deposition and remodeling. This process has been called “ligamentization” since the end product grossly, histologically and biochemically resembles a normal ACL. Experimental data indicates that autograft and allograft tissues are revascularized by vessels from the soft tissues (fat pad and synovium), the drilled bone tunnels, and the synovial fluid.
The work of Amis et a1. indicates that the graft is repopulated by cells of extrinsic origin. They postulated that these extrinsic cells were derived from undifferentiated synovial cells (Type C cells). These extrinsic undifferentiated cells re-establish the cellular matrix of the graft. In the proper mechanical environment, the repopulated graft matures and remodels. This process of “ligamentization” takes from 6 9 months in experimental animal models, and perhaps longer in humans. Attempts at maintaining the vascular supply to the graft have failed to accelerate this process.
During the period of necrosis, revascularization, repopulation, collagen deposition and remodeling, the autograft undergoes a dramatic change in it’s mechanical properties. Animal experiments have shown that autografts demonstrate a rapid drop in mechanical strength, between 6 8 weeks following implantation, having only approximately 50% of their initial mechanical strength at this time. Following this rapid drop in strength, autografts show a slow but steady increase in their tensile properties. In a Rhesus monkey model, Clancy et a1. showed a return to 80% of the initial tensile strength of a patellar tendon graft at 12 months. But no study has ever shown a complete return to the initial mechanical strength of the transplant.The important point to remember is that since the autograft will never recover 100 % of its initial mechanical strength, autografts are strongest at the time that they are implanted:
The work of Jackson et a1., Oakes et al., and Abe et al. may provide a explanation for the loss in tensile strength of autograft tissue following implantation. Jackson et al. used in situ freeze thaw model to simulate an ideally placed and oriented autogenous ACL graft. At 26 weeks, there were no statistically significant differences between the treated ligament and the control untreated ligaments relative to A P translation, maximum force to rupture, linear stiffness, and modulus of elasticity. These observations were in sharp contrast to previous studies in which an allograft of the ligament, and a LAD augmented allograft were used to replace the ACL. In these previous studies, the maximum strength at 1 year was 75% for the allograft, and 50° for the allograft augmented with a LAD. They concluded that with proper placement, orientation and tension, devitalized, devascularized ACL ligaments do not necessarily lose their mechanical properties. The implications of this work is that with proper placement and tension, transplanted graft tissue does not necessarily undergo a marked loss of tensile strength.
Ultrastructural studies have shown that large diameter collagen fibril (>100 nm) form a large proportion (45%) cross¬sectional area of the normal human patellar tendon, while approximately 85% of the cross sectional area of the human ACL is composed of collagen fibrils less than 100 nm in diameter. Oakes has speculated that it is these large diameter collagen fibers that may explain the high ultimate failure loads of the patellar tendon.
Biopsy studies of autogenous ACL grafts(patellar tendon, hamstring tendons and allografts by Oakes and Abe et al., have shown a striking loss of the large diameter (> 100 nm) collagen fibrils, and a loss of the tight packing of the fibers seen in the normal ACL. These findings were noted irrespective of the autograft tissue implanted. One explanation for the loss of the large diameter collagen fibrils following ACL replacement, is that although the autograft tissue is repopulated by fibroblasts derived from stem cells of the synovium (Type C cells), these synovial derived fibroblasts are not capable of synthesizing the large diameter collagen fibrils seen in the normal ACL and patellar tendon. Synovial cells are known to synthesize hyaluronate, which has been shown in bovine and chick models to favor the production of small diameter collagen fibrils. This loss of large diameter collagen fibrils in transplanted autograft tissue may explain SOME of the loss in tensile strength of autograft tissues following implantation.
Although allografts undergo the same biological response as autografts, there is some experimental evidence that the decrease in mechanical properties in allografts is greater than that seen in autograft tissue, and that allograft tissues seem to incorporate much slower than autograft tissue. Since both autograft and allograft tissue show the same loss of mechanical strength, this underscores the importance of using grafts with initial mechanical properties greater than that of the normal ACL.
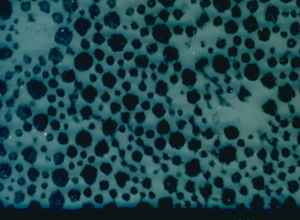
Normal ACL Collagen Fibres under Electron Microscope shows
Large Collagen Fibres
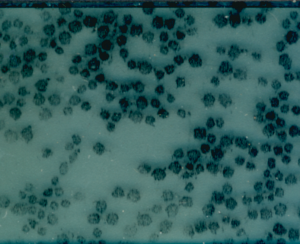
12 months Allograft shows smaller Collagen Fibres
Graft Placement
The objectives of intra articular replacement of the ACL are to replicate the normal anatomy and function of the ACL as closely as possible. A major goal of surgical placement of ACL grafts has been to try to locate attachment sites on the femur and tibia that have no change in length with flexion and extension of the knee, so called “isometric” placement . The primary objective of isometric placement is to prevent excessive elongation or slackening of the graft as the knee is flexed and extended from the position where the graft is tensioned and fixed. Non isometric placement can lead to large graft forces which can result in permanent deformation failure of the graft tissue. Non isometric placement can lead to large graft forces which can “capture” the knee joint leading to a loss of joint motion and altered joint kinematics.
It is important to recognize that the normal ACL is not isometric since each ACL ligament fiber has a unique attachment site and tension. Arms et al. and Sapega et al. have shown that the so called “anteromedial fibers” of the human ACL undergo the smallest changes in length with flexion and extension of the knee. Based on these studies, most surgeons feel that the intra operative goal of ACL surgery is to replicate the strain pattern of the anteromedial fibers.
Biomechanical studies have shown that isometry of ACL substitutes is most sensitive to femoral tunnel placement . The most “isometric” region is located posterior and superior in the intercondylar notch, 3 5 mm anterior to the “over the top” position on the lateral wall.
What are the consequences of incorrect graft location? Substitutes placed anterior to the isometric region tend to lengthen with knee flexion, leading to either a restriction of knee flexion or rupture or stretching of the substitute as knee flexion is gained.
The posterolateral bundle is less isometric and for that reason it often tears in case of double bundle ACL Reconstruction.
Graft length changes are much less sensitive to tibial hole placement. Anterior posterior tibial placement primarily determines graft impingement in the notch with extension. Work by Dr. Stephen Howel1 using MRI imaging of postoperative ACL grafts has shown that placement of the tibial guide pin at the anteromedial location as advocated by Clancy et al., will result in impingement of the ACL graft in the roof of the intercondylar notch. Clinically this is manifested by pain, swelling, an inability to achieve full extension, and quadriceps weakness. This roof impingement is difficult to detect at the time of surgery. Using serial postoperative MRI studies Howell has been able to show that following implantation, hamstring and patellar tendon autografts have a low signal black homogeneous appearance. By 3 months postoperative, an impinged graft has an area of high signal intensity at the distal third of the graft. This high signal intensity presumably represents edema and swelling of the graft. On a plain lateral radiograph with the knee in maximum extension, a portion of the tibial tunnel was noted to be anterior to the roof of the intercondylar notch in impinged grafts. If the eccentric anteromedial tibial tunnel position as recommended by Clancy was used, then on average 5.0 mm of bony resection from the roof of the intercondylar notch be removed to prevent impingement of the ACL graph in extension. A more “posterior” tibial tunnel placement 3 mm posterior to the center of the ACL requires minimal bony resection from the notch. Howell was also able to show that by performing a “delayed roofplasty” and raising the roof of the notch such that the tibial tunnel was posterior to the new roof position, it would allow the MRI signal of an impinged graft to return to normal. This information suggests that the sagittal position of the tibial tunnel is a critical determinate of roof impingement. Medial lateral tibial guide pin placement determines impingement along the lateral femoral condyle with knee flexion. Staeubli from Switzerland could show, that roof impingement can be avoided by placing the centre of the tibial tunnel at the 43 % mark of the a.p. diameter. This mark is used in computer navigated surgery.
Graft tension
Little is known about the effects of initial graft tension on remodeling of biological ACL substitutes. The study by Yoshiya et al. suggests that over tensioning the substitute may impair remodeling of biologic substitutes. Over tensioning the substitute could lead to an over constrained joint, resulting in excessive stress on the substitute, or excessive shear stresses on the articular cartilage. An over constrained joint may also limit ROM.
It is important to avoid over constraining the joint as this can result in a loss of motion or generate excessive compressive loads on the articular cartilage. Bylski Austrow et a1. showed that the angle of the knee at the time of tensioning was more important than the actual tension applied to the ligament, in avoiding overconstraint of the joint. Grafts tensioned at 30° were more likely to result in posterior overcontraint of the joint, than grafts tensioned at 0°. This study suggest that ACL grafts should be tensioned in full extension. This applies in particular to BTB grafts as they are stiffer than the normal ACL! In one of the discussions of the European Society of Sports Medicine meetings a tension of 60 Newton was thought to be a reasonable tension to fix the graft with.
Graft fixation
Rigid fixation of the ACL substitute to bone is probably one of the major factors influencing the stability and success of ACL surgery in the immediate postoperative period. In fact, in the immediate postoperative period, rehabilitation limitations are based more on considerations of graft fixation, than graft strength. Studies by Daniel and Robertson have shown the weakness of suture and staple fixation of soft tissue substitutes to bone. Stronger fixation strength was obtained with spiked ligament washers and plates.
For bone tendon bone substitutes, Kurosaka et al. have shown the advantages of interference screw fixation. Of note is that none of the current fixation methods can achieve fixation strengths equal to the failure strength of the patellar tendon graft, or the normal ACL.
Fixation devices like the endobutton CL (1100N)for the femur and Intrafix for the Tibia (1100N, AAOS 2000) provide even stronger soft tissue fixations for the hamstrings (more than double the strength of patellar tendon graft fixation with screws !).
Most studies have also shown that for both hamstring and patellar tendon grafts, the weakest point of the construct is the tibial fixation site. For that reason I often use an additional ligament staple on the tibial side in addition to an interference screw.
Surgical Options
Single vs Double Bundle Reconstruction
Primary repair of the ACL alone yields very unpredictable results and an unacceptably high failure rate.
Therefore, the current surgical recommendations for the acute ACL are primary reconstruction of the ACL with a high strength graft.
Double bundle Reconstruction was popular in the late 1990 (I was one of the first double bundle surgeons in Germany at the Arcus Sports Clinic in 1998) , but over time it has become unpopular.
In an effort to attempt an anatomical replacement of the ACL, the idea is to use 2 bundles instead of one bundle. This is to recreate the band like flat insertion site on the femur and the C-shaped insertion on the Tibia. It was hoped the knees were tighter , there would be less re-ruptures and there would be better long term outcomes. Two tunnels for the Tibia and two tunnels for the Femur are used . The AMB (anteromedial bundle) stabilizes AP laxity in deep flexion , The PLB (postero lateral bundle) controls AP laxity in 0-30 flexion (Rotation, Pivot).
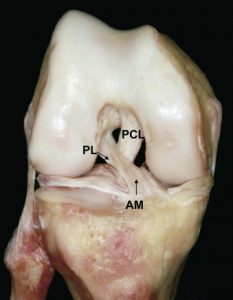
Knee Anatomy (PL=Postero Lateral, AM=Antero-Medial)
PCL(Posterior Cruciate Ligament)
Femoral ACL insertion (supplied by R Siebold, ATOS Clinic)
X ray imaging of femoral ACL insertion
C shaped tibial insertion of ACL
Length 12,6mm, width 3,3mm (supplied by R Siebold, ATOS Clinic)
The surgical impact is to use a “central bone tunnel” and do a flat reconstruction (PT, QT, DB Hamstrings) on the femur and to attempt to reconstruct the C shaped of footprint on the Tibia.
Reconstruction of C shape with AM and PM bone tunnel placement
Unfortunately, studies revealed that the Double bundle Reconstruction did not provide better long term outcomes as expected.
The risks of surgery and the complication rates are higher for the double bundle and this outweighs the possible benefit in stability.
At the ACL study group meeting in Cape town 2014, Andrew Amis showed that the role of different ACL fibres is not equivalent. He came to the conclusion that a small percentage of fibres play a major role (tibial AM bundle).
In summary a well placed single bundle ACL recon works well for most patients. Additional, stability may be provided by an extra-articular tenodesis.
I see little place for double bundle procedures.
Remnant Preservation
Preserving the ruptured ACL tibial remnant makes a lot of sense.
The tibial stump is full of vascularity , nerve fibres and healing cells, which can contribute to the Ligamentization (healing process) of the new ACL reconstruction.
Arthroscopic picture of new ACL construct surrounded by tibial stump (torn tibial ACL remnant).
In case of isolated bundle ruptures (AMB or PMB) each bundle can be reconstructed individually , whilst preserving the intact bundle.
By preserving the tibial stump, there are multiple benefits:
- Gohill (2006) showed faster Ligamentization.
- Adachi (Level III) showed better proprioception.
- Annear revealed earlier return to normal MRI signal.
And there is no downside.
In conclusion the tibial stump should be preserved at the time of ACL Reconstruction as this has shown to improve outcome.
Extra articular (ALL/Antero lateralLigament Reconstruction )
Biomechanical studies have confirmed that the ACL is the primary restraint to anterior tibial translation, and is the vital link in the 4 bar linkage system which determines normal knee kinematics. Because extra articular procedures fail to restore the critical “central pivot” and normal knee kinematics, most surgeons have completely abandoned primary extra articular procedures in favor of intra articular reconstruction of the ACL. What about combined intra articular extra articular reconstruction? It is also used for high level sports soccer players and for revision cases. So far there is limited evidence, that an ALL reconstruction combined with an ACL Reconstruction has any advantage to an intra ¬articular ACL reconstruction. At present most surgeons perform an intra articular reconstruction with a high strength graft in chronic and acute cases.
Timing of Acute Surgery
Studies by Strum, Shelbourne and Harner have shown that acute ACL surgery performed within 2 weeks of the ACL tear are associated with a much higher incidence of knee stiffness, compared to surgery which is delayed until a good Range of Motion has been achieved. Thus surgery can be delayed, giving the patient time to achieve full motion and return of muscle strength prior to undergoing reconstruction. This approach has resulted in a significant reduction in the incidence of loss of motion. There are other studies, that suggest early surgery is safe and provides favorable outcomes. By the end of the day each case has to be treated individually. Significant preoperative stiffness is certainly a contraindication for immediate surgery.
Treatment of Combined ACL/MCL/LCL Injuries
Studies by Shelbourne and Basle, and Harner et a1. have documented a particularly high incidence of loss of knee motion following ACL reconstruction with operative repair of the MCL. In an effort to minimize this complication, the current trend for combined ACL/MCL injuries is to treat the MCL injury non¬operatively, and then perform ACL reconstruction on a delayed basis. A report by Shelbourne and Porte has shown that this approach can result in excellent anterior and valgus stability, with a normal range of motion.
Non operative treatment of Grade III MCL tears is currently recommended only for medial side injuries involving the superficial MCL. This implies that the knee should be stable to valgus stress in the hyperextended position and in the 0° extension position. If there is significant medial compartment opening in the hyperextended position, or at 0°, then one is dealing with more than injury to the superficial MCL. The posterior capsule, and POL are also involved. For this type of injury, surgical repair or reconstruction of the MCL is recommended.
For severe Valgus stress injuries with complete rupture of MCL and PCL ,I prefer to treat the PCL non operatively but reconstruct the MCL using a 4x Hamstring Graft.
Combined ACL, lateral and posterolateral injuries are treated by early reconstruction of the ACL, and repair or reconstruction of the lateral and posterolateral structures.
Return to Sport after ACL Reconstruction
Return to Sport is influenced by-
preoperative factors (age, pre- op rehab , knee stiffness & neuromuscular control), intraoperative (graft choice, positioning and fixation ) as well as postoperative (psychological factors , rehabilitation & lower limb strength/ functional symmetry).
Thomee showed that failure to regain muscle strength and function is a major reason contributing to patients inability to RTS as well as increasing the risk of re-rupture.
The best and most commonly reported objective Criteria to determine readiness to RTS are the single Hop for distance & isokinetic strength testing (as described by Barber Westin 2011)
This is best reported via Limb Symmetry Indices , a measure of the strength and function of the operated limb compared to the healthy non operated side . Achieving 90% of function compared to the healthy leg is determined to be satisfactory .
![]()
![]()
In 2016, Kyritsis had a 17% re-rupture rate after ACL recon – associated with not meeting the objective cut offs (being more than 90% limb symmetry indices for isokinetic Quads strength and functional hop symmetry)
Grindem showed that in the patients that had achieved a RTS :
There was a 5% re- tear rate if Quad/ham strength and hop capacity was more than 90% and a 40% re-tear rate if quad /ham strength &hop capacity was less than 90% of opposite leg.
Looking at our own patients in collaboration with J.Ebert (Hollywood functional Rehab centre), we determined that adequate rehabilition including agility and landing exercises correlated strongly with Strength and Hop symmetry.
A test battery was developed and we find this a very useful tool to help decide if a patient is ready to return to sport. A low test score is a good argument to delay RTS. Usually the Return To Sport test battery is not attempted before the 9-12 months mark post-operatively.
RTS testing is recommended for all Level I sports, in particular all ball sports. Return to ball sports and martial arts is generally not recommended before 1 year post surgery.