The shoulder joint is the most mobile and flexible joint of the body, however it is also highly vulnerable to injury. Shoulder instability is common in the young sporting population.
Stability to the shoulder is provided by the labrum, which encircles the glenoid and the various ligaments, which attach to it. Tears of the labrum and the attached ligaments (gleno-humeral ligaments) result in instability.
Anterior dislocation is the most common form of instability. Often it is the result of an acute injury, which causes detachment of the labrum from the anterior glenoid. Posterior, Superior (SLAP tears) and multidirectional instabilities with detachment of the labrum elsewhere are less common.
Shoulder Arthroscopy
I usually perform arthroscopic stabilisation surgery. By using the arthroscope either through anterior or posterior portals the labrum with it’s capsule/ligament complex can be repaired in all locations. No additional incisions are required. The torn tissue is anatomically repaired. With this procedure there is less scarring and less loss of range of motion, compared to open procedures. Success rates are equal to open procedures.
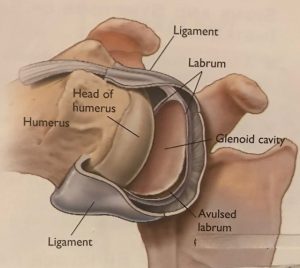
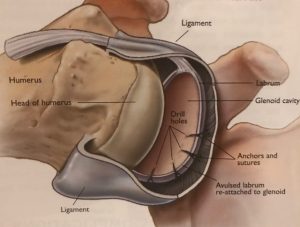
Torn labrum (left) and after repair (right)
Shoulder Stabilisation Post-Operation
Cave: To allow the labrum to heal it is most important to keep the arm in a sling in the first 4 (-6) weeks. Excessive shoulder movement early after surgery can lead to joint fluid penetrating between the repaired labrum and the glenoid, which prevents it from healing.
If the healing does not occur in the early post-operative period, the long term outcome will not be as good as expected and a re-injury (re-dislocation) becomes more likely.